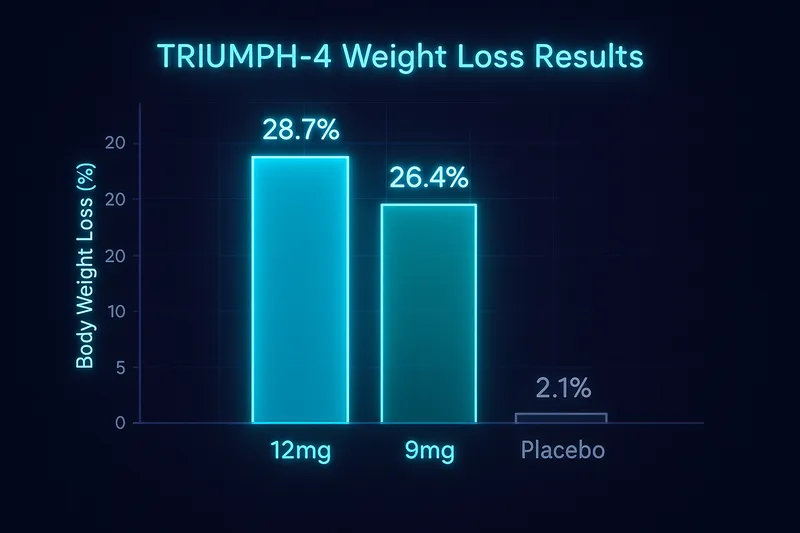
The obesity treatment landscape just shifted again. Eli Lilly's TRIUMPH-4 trial — a global, randomized, placebo-controlled Phase III study — has delivered results that surpass anything previously seen in obesity pharmacotherapy. Participants receiving the 12 mg dose of retatrutide lost an average of 28.7% of their body weight over 68 weeks, roughly 71.2 pounds. That figure eclipses existing incretin-based therapies and brings pharmacological weight loss into territory once reserved for bariatric surgery.
But TRIUMPH-4 wasn't just about the scale. The trial also demonstrated dramatic improvements in knee osteoarthritis pain, reductions in cardiovascular risk markers, and a safety profile consistent with prior incretin receptor agonist data. Here's what the results mean and why they matter.
What Is Retatrutide?
Retatrutide (LY3437943) is an investigational peptide developed by Eli Lilly that acts on three distinct hormone receptors simultaneously: glucose-dependent insulinotropic polypeptide (GIP), glucagon-like peptide-1 (GLP-1), and glucagon receptors. This triple agonist mechanism distinguishes it from existing therapies like semaglutide (a GLP-1 receptor agonist) and tirzepatide (a dual GIP/GLP-1 receptor agonist).
Each receptor pathway contributes a distinct physiological effect:
- GLP-1 receptor activation reduces appetite, slows gastric emptying, and enhances insulin secretion — the mechanism behind semaglutide and the GLP-1 component of tirzepatide.
- GIP receptor activation works synergistically with GLP-1 signaling to amplify insulin response and may independently influence fat metabolism. This dual approach is what gives tirzepatide its edge over single-agonist GLP-1 therapies.
- Glucagon receptor activation — the novel addition in retatrutide — increases energy expenditure, promotes hepatic fat oxidation, and may enhance thermogenesis. This is the pathway that theoretically pushes weight loss beyond what dual agonists can achieve.
For a deeper look at how retatrutide works and its dosing protocols, see our retatrutide dosing guide.
The Phase II data (published in The New England Journal of Medicine in 2023) already hinted at retatrutide's potential, showing up to 24.2% weight loss at 48 weeks at the highest dose tested (Jastreboff et al., NEJM 2023). TRIUMPH-4 was designed to confirm and extend those findings in a larger, longer, and more diverse Phase III population.
TRIUMPH-4 Trial Design
TRIUMPH-4 was a global, randomized, double-blind, placebo-controlled Phase III trial enrolling adults with obesity or overweight with at least one weight-related comorbidity. Key design features included:
- Duration: 68 weeks of treatment
- Doses tested: 9 mg and 12 mg retatrutide, administered once weekly via subcutaneous injection
- Comparator: Matched placebo
- Primary endpoints: Percent change in body weight from baseline; proportion of participants achieving ≥5% weight loss
- Key secondary endpoints: Proportion achieving clinically meaningful weight loss thresholds (≥10%, ≥15%, ≥20%, ≥25%, ≥30%, ≥35%), changes in cardiometabolic risk markers, and patient-reported outcomes including knee osteoarthritis pain
The trial is part of Lilly's broader TRIUMPH clinical program, which encompasses multiple Phase III studies evaluating retatrutide across different populations and comorbidities.
Weight Loss Results: Unprecedented Numbers
The headline numbers from TRIUMPH-4 are striking by any standard.
Mean Body Weight Reduction
| Group |
Mean Weight Loss (%) |
Approximate Pounds Lost |
| Retatrutide 12 mg |
28.7% |
~71.2 lbs |
| Retatrutide 9 mg |
26.4% |
~65.5 lbs |
| Placebo |
2.1% |
~5.2 lbs |
To put these numbers in context: semaglutide 2.4 mg (the highest approved dose for obesity) produced approximately 15–17% weight loss in the STEP trials (Wilding et al., NEJM 2021). Tirzepatide at its highest dose (15 mg) achieved approximately 22.5% in the SURMOUNT-1 trial (Jastreboff et al., NEJM 2022). Retatrutide's 28.7% represents a meaningful step beyond both.
Categorical Weight Loss Thresholds
What makes the TRIUMPH-4 data particularly remarkable is the proportion of participants reaching aggressive weight loss targets:
- ≥25% body weight loss — achieved by a high proportion of participants in both active-dose arms, a threshold rarely reached in pharmacotherapy trials
- ≥30% body weight loss — a substantial number of participants crossed this threshold, which approaches outcomes seen with some bariatric surgical procedures
- ≥35% body weight loss — even at this extreme threshold, a meaningful proportion of the 12 mg group achieved it
These categorical results matter clinically because greater degrees of weight loss are associated with more robust improvements in obesity-related comorbidities, including type 2 diabetes remission, obstructive sleep apnea resolution, and cardiovascular risk reduction.
Beyond the Scale: Knee Osteoarthritis Pain Relief
One of the most clinically significant — and perhaps underappreciated — findings from TRIUMPH-4 was the effect on knee osteoarthritis symptoms. Obesity is a primary driver of knee osteoarthritis, and weight loss has long been recommended as first-line therapy. But the magnitude of pain improvement in TRIUMPH-4 went beyond what weight loss alone would typically predict.
WOMAC Pain Scores
The trial assessed knee osteoarthritis pain using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), a validated instrument widely used in orthopedic and rheumatologic research.
- Baseline WOMAC pain score: approximately 6 out of 20
- Reduction in active treatment arms: approximately 4.5 points, representing a ~76% decrease from baseline
- Complete freedom from knee pain at week 68: reported by roughly 1 in 8 patients (12.5%) receiving retatrutide, compared to just 4.2% in the placebo group
A 76% reduction in pain scores is extraordinary — approaching the range typically seen after total knee replacement surgery. A once-weekly injection delivering that level of pain relief in patients who may not yet need surgery is a potentially transformative finding.
The mechanism likely involves both the direct mechanical benefit of reduced joint loading (less body weight pressing on the knee) and possible anti-inflammatory effects mediated through reductions in systemic inflammation — a known consequence of significant weight loss and potentially enhanced by glucagon receptor-mediated metabolic improvements.
Cardiovascular Risk Markers
TRIUMPH-4 also assessed a panel of cardiometabolic biomarkers, and the results were broadly favorable across the board:
- Non-HDL cholesterol — significant reductions, indicating improved atherogenic lipid burden
- Triglycerides — meaningful decreases, consistent with the known effects of GLP-1 and GIP receptor activation on lipid metabolism
- High-sensitivity C-reactive protein (hsCRP) — substantial reductions, reflecting decreased systemic inflammation. Elevated hsCRP is an independent cardiovascular risk factor, and its reduction is considered a surrogate marker for improved cardiovascular outcomes
- Systolic blood pressure — clinically meaningful reductions
These improvements are consistent with — but in several cases exceed — the cardiometabolic benefits observed with semaglutide and tirzepatide in their respective Phase III programs. Whether retatrutide's glucagon receptor agonism provides additive cardiovascular benefit beyond what GLP-1 and GIP activation deliver is an important question that dedicated cardiovascular outcomes trials (CVOTs) within the TRIUMPH program may eventually answer.
The cardiometabolic data also reinforce the emerging understanding that incretin-based therapies produce benefits beyond weight loss itself — likely through direct receptor-mediated effects on hepatic metabolism, vascular inflammation, and lipid handling.
Safety Profile
The safety data from TRIUMPH-4 were consistent with the known class effects of incretin receptor agonists, with no unexpected signals emerging at either dose.
Gastrointestinal Side Effects
The most common adverse events were gastrointestinal in nature, as expected for this drug class:
- Nausea — the most frequently reported GI side effect, typically most pronounced during dose escalation and diminishing over time
- Diarrhea — reported at moderate frequency
- Constipation — less common than nausea but clinically relevant for some participants
- Vomiting — generally mild and often transient
These GI effects are mechanistically linked to GLP-1 receptor activation (slowed gastric emptying, central appetite suppression) and are a recognized feature of all GLP-1-based therapies. The dose escalation protocol used in TRIUMPH-4 was designed to mitigate their severity, and most events were mild to moderate in intensity.
Dysesthesia
A notable finding was dysesthesia (an abnormal sensation such as tingling, burning, or numbness), reported in up to 20.9% of participants at the 12 mg dose. This side effect was generally described as mild and was first identified in the Phase II program. The mechanism is not fully understood but may relate to glucagon receptor-mediated effects or rapid metabolic changes associated with significant weight loss. Importantly, dysesthesia rarely led to treatment discontinuation and tended to resolve or stabilize over time.
Overall Tolerability
The overall discontinuation rate due to adverse events remained within the range observed for semaglutide and tirzepatide in their respective programs. The benefit-risk profile at both the 9 mg and 12 mg doses appears favorable, though individual tolerability will vary — as it does with all incretin-based therapies.
For patients and clinicians, the practical takeaway is that retatrutide's side effect profile is broadly similar to existing peptide-based obesity treatments, with the addition of dysesthesia as a novel but generally manageable consideration.
What This Means for Patients
TRIUMPH-4 is a landmark trial, but it's important to contextualize what these results mean for people living with obesity today.
Retatrutide is not yet approved. The TRIUMPH-4 data are part of an ongoing Phase III program, and regulatory submissions to the FDA and other agencies have not yet been completed. Approval, if it comes, is likely still at least 12–18 months away, depending on the pace of remaining readouts and regulatory review.
The results apply to a clinical trial population. Participants in Phase III trials are carefully selected and monitored, receive structured dose escalation, and have regular clinical follow-up. Real-world results may differ — though the consistency of incretin-based therapy data across trials and post-marketing settings is encouraging.
Weight loss of this magnitude has cascading health benefits. Losing nearly 29% of body weight doesn't just improve how someone looks or feels — it meaningfully reduces the risk of type 2 diabetes, cardiovascular disease, obstructive sleep apnea, non-alcoholic fatty liver disease, and certain cancers. For patients with knee osteoarthritis, the pain relief demonstrated in TRIUMPH-4 could mean the difference between mobility and disability.
Individual results will vary. As with semaglutide and tirzepatide, some patients will be high responders and others will experience more modest effects. Genetic factors, adherence, diet, physical activity, and baseline metabolic health all influence treatment response.
For more on how retatrutide fits into the current landscape, visit our comprehensive retatrutide profile.
How Retatrutide Compares to Existing Therapies
The progression from single to dual to triple agonist therapy represents a clear trend in obesity pharmacotherapy:
- Semaglutide (GLP-1 agonist): ~15–17% weight loss in Phase III (STEP trials)
- Tirzepatide (GIP + GLP-1 dual agonist): ~20–22.5% weight loss in Phase III (SURMOUNT trials)
- Retatrutide (GIP + GLP-1 + glucagon triple agonist): ~26–29% weight loss in Phase III (TRIUMPH-4)
Each additional receptor pathway appears to contribute incremental efficacy. The glucagon receptor component in retatrutide likely drives the additional weight loss through increased energy expenditure and enhanced hepatic fat metabolism — mechanisms not directly targeted by GLP-1 or GIP activation alone.
However, more receptors also means more pharmacological complexity. The dysesthesia signal in retatrutide, while mild, is an example of a novel side effect that wasn't seen with simpler agonists. Long-term safety data — particularly cardiovascular outcomes and effects on lean body mass — will be critical for fully understanding retatrutide's place in therapy.
For a detailed head-to-head comparison of the current leading peptide therapies, see our semaglutide vs. tirzepatide comparison.
What's Next: The TRIUMPH Program and Regulatory Path
TRIUMPH-4 is just one piece of a much larger puzzle. Lilly's TRIUMPH clinical program includes multiple Phase III trials evaluating retatrutide across different patient populations and endpoints:
- Seven additional Phase III readouts are expected throughout 2026, covering populations with type 2 diabetes, cardiovascular disease, obstructive sleep apnea, and other obesity-related comorbidities
- Cardiovascular outcomes data — the gold standard for demonstrating that weight loss translates into reduced heart attacks, strokes, and cardiovascular death — will be critical for retatrutide's regulatory and commercial positioning
- Head-to-head trials comparing retatrutide directly to existing therapies may provide definitive comparative efficacy data
The Drug vs. Biologic Question
An important regulatory subplot is Lilly's appeal of the FDA's classification of retatrutide. The company is challenging whether retatrutide should be classified as a drug or a biologic — a distinction with significant implications for compounding.
Under current FDA rules, drugs listed on the Drug Shortage List may be compounded by 503A and 503B pharmacies, while biologics face stricter restrictions. This classification question has already been contentious for semaglutide and tirzepatide, and Lilly appears to be proactively seeking a regulatory framework that may limit compounding of retatrutide from the outset. The outcome of this appeal could shape patient access and pricing dynamics for years to come.
Timeline to Approval
Based on the expected cadence of remaining TRIUMPH readouts and standard FDA review timelines, the earliest possible U.S. approval for retatrutide in obesity would likely be in late 2027 or 2028, though an accelerated pathway is possible if the totality of evidence is sufficiently compelling. Regulatory submissions in other markets (EU, UK, Japan) would follow on a similar or slightly delayed timeline.
The Bottom Line
TRIUMPH-4 establishes retatrutide as the most potent pharmacological weight loss agent ever tested in a Phase III program. A 28.7% average weight loss at 68 weeks — coupled with transformative improvements in knee osteoarthritis pain, cardiovascular risk markers, and metabolic health — represents a genuine advance in obesity treatment.
The triple agonist mechanism appears to deliver on its theoretical promise: each additional receptor pathway contributes measurable clinical benefit. Whether those benefits are sustained long-term, whether the safety profile holds up across larger and more diverse populations, and whether the drug-vs-biologic classification battle shapes patient access — these are the questions that 2026's remaining TRIUMPH readouts will begin to answer.
For now, the data speak clearly. Retatrutide works, and it works at a level that would have been considered unrealistic just five years ago. Compare current retatrutide vendors and pricing on our retatrutide buying guide.
Frequently Asked Questions
How much weight can you lose on retatrutide?
In the TRIUMPH-4 Phase III trial, participants on the 12 mg dose lost an average of 28.7% of their body weight (~71 lbs) over 68 weeks. The 9 mg dose produced 26.4% average loss. Individual results vary based on baseline weight, adherence, diet, and activity level. For dosing details, see our retatrutide dosing guide.
Is retatrutide better than semaglutide or tirzepatide?
Based on Phase III data, retatrutide produces significantly more weight loss than both semaglutide (~15–17%) and tirzepatide (~22.5%). The key difference is retatrutide's third receptor — glucagon — which increases energy expenditure and fat oxidation. However, retatrutide is not yet FDA-approved, while semaglutide and tirzepatide are available now. See our semaglutide vs tirzepatide comparison for more.
When will retatrutide be available?
Retatrutide is still in Phase III trials. Based on remaining TRIUMPH program readouts (7 more expected in 2026) and standard FDA review timelines, the earliest possible U.S. approval would be late 2027 or 2028. Research-grade retatrutide is available from peptide vendors — compare prices here.
What are the side effects of retatrutide?
The most common side effects are gastrointestinal: nausea, diarrhea, constipation, and vomiting — similar to other GLP-1 therapies. A unique finding is dysesthesia (tingling/numbness), reported in up to 21% of participants at the 12 mg dose, though generally mild. See the safety profile section above for the full breakdown.
How does retatrutide work differently from other weight loss peptides?
Retatrutide is the first triple agonist — it activates GIP, GLP-1, and glucagon receptors simultaneously. Semaglutide targets only GLP-1, while tirzepatide targets GIP + GLP-1. The glucagon receptor adds increased energy expenditure and hepatic fat oxidation, which appears to drive the additional weight loss beyond what dual agonists achieve.
Can retatrutide help with conditions other than obesity?
TRIUMPH-4 showed significant benefits for knee osteoarthritis pain (76% reduction) and cardiovascular risk markers (cholesterol, triglycerides, blood pressure, inflammation). Additional Phase III trials are evaluating retatrutide for type 2 diabetes, obstructive sleep apnea, and other metabolic conditions.
References
| Citation |
Topic |
| Lilly TRIUMPH-4 press release (February 2026) |
Phase III topline results |
| Jastreboff AM et al., N Engl J Med 2023; 389:514-526 |
Retatrutide Phase II obesity trial |
| Wilding JPH et al., N Engl J Med 2021; 384:989-1002 |
Semaglutide STEP trial results |
| Jastreboff AM et al., N Engl J Med 2022; 387:327-340 |
Tirzepatide SURMOUNT-1 trial |
This article is for educational purposes only and does not constitute medical advice. Retatrutide is an investigational compound not yet approved by the FDA or any regulatory agency. Consult a healthcare provider for personalized treatment guidance.