Tesofensine is an oral small-molecule triple monoamine reuptake inhibitor — not a peptide — used for weight loss. For the full mechanism and clinical trial data, see our tesofensine weight loss guide.
Not FDA-approved. All protocols below are based on Phase II clinical trial data and community experience. This is not medical advice.
| Parameter |
Community Protocol |
| Compound type |
Small molecule (not a peptide) |
| Route |
Oral (capsule) |
| Starting dose |
0.25 mg/day for 1-2 weeks |
| Standard dose |
0.5 mg/day |
| Timing |
Morning, fasted or with light meal |
| Frequency |
Once daily |
| Cycle |
8 weeks on, 4 weeks off |
| Half-life |
~220 hours (parent compound) |
| Storage |
Room temperature |
Start at 0.25 mg daily for 1-2 weeks to assess tolerance, then increase to 0.5 mg daily. The 0.5 mg dose provides ~88% of the maximum clinical effect with significantly fewer side effects than 1.0 mg.
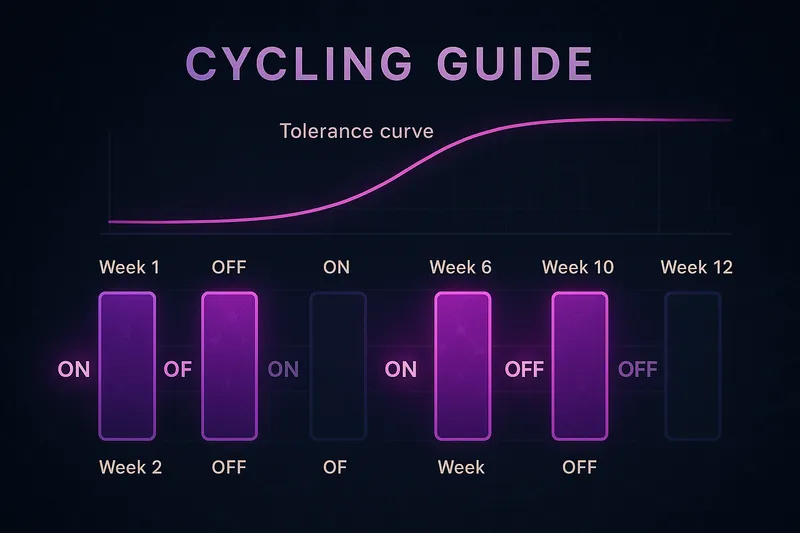
Cycling Details
Tesofensine's monoamine mechanism means tolerance is a real consideration. The standard approach is 8 weeks on, 4 weeks off.
Signs tolerance is developing (typically weeks 4-6): appetite suppression weakening, energy boost diminishing, return of cravings. If you notice these, cycle off — do not increase the dose.
Alternative: 5on/2off weekly — 5 days on (Mon-Fri), 2 days off (weekends), continuing for 10-12 weeks before a full 4-week break. However, given the ~220-hour parent compound half-life, the 2-day break may not provide meaningful receptor recovery. The standard 8/4 cycle is more effective for managing tolerance.
Routes of Administration
Oral (only route): Swallow capsule whole in the morning. Fasted or with a light meal — absorption is not significantly affected by food, but some users report faster onset fasted. Take at the same time daily.
No reconstitution needed. Not an injectable.
Where These Numbers Come From
The landmark Phase II trial (TIPO-1) tested three doses against placebo over 24 weeks with a controlled diet:
| Dose |
Weight Loss |
vs Placebo |
| 0.25 mg |
6.7% |
Significant |
| 0.5 mg |
11.3% |
Highly significant |
| 1.0 mg |
12.8% |
Highly significant |
The jump from 0.25 mg to 0.5 mg was substantial (nearly double), while 0.5 mg to 1.0 mg gained only 1.5 percentage points with far more side effects. This dose-response curve is why the community settled on 0.5 mg (Astrup et al., 2008).
Sjödin et al. (2010) showed tesofensine increased energy expenditure and reduced appetite through triple monoamine reuptake inhibition — dopamine, serotonin, and norepinephrine (Sjödin et al., 2010).
Stacking Protocols
Tesofensine + GLP-1 Agonist
| Compound |
Dose |
Route |
Purpose |
| Tesofensine |
0.5 mg daily |
Oral |
Appetite suppression via DA/NE/5-HT, energy expenditure |
| Semaglutide or Tirzepatide |
Per protocol |
SC |
Satiety via GLP-1, gastric emptying |
Completely different mechanisms — some users report more effective appetite control than either alone. Keep both at moderate doses since combined suppression can be strong.
What NOT to Stack
Never combine with: MAOIs (serotonin syndrome risk), SSRIs/SNRIs (serotonergic overlap), stimulants (amphetamines, methylphenidate, modafinil), or other monoamine reuptake inhibitors (sibutramine, bupropion).
Side Effects & Safety
At 0.25 mg: Mild dry mouth, slight sleep difficulty if taken late, occasional headache, mild heart rate increase (2-5 bpm).
At 0.5 mg: Dry mouth (most common), insomnia (dose early, before 9am), elevated heart rate (5-10 bpm), constipation, mild mood elevation.
At 1.0 mg (not recommended): Significant heart rate increase (8-15+ bpm), more frequent insomnia, anxiety/jitteriness, nausea, mood swings.
Drop dose or stop if: Resting heart rate consistently above 100 bpm, persistent insomnia beyond one week, significant anxiety, palpitations, or blood pressure spikes.
Contraindicated: Cardiovascular disease, uncontrolled hypertension, history of stroke, arrhythmias, glaucoma, hyperthyroidism, seizure history.
Frequently Asked Questions
What is the standard tesofensine dose?
0.5 mg orally once daily in the morning. Start at 0.25 mg for 1-2 weeks to assess tolerance, then increase. Cycle 8 weeks on, 4 weeks off.
How long does it take for tesofensine to start working?
Appetite suppression within 2-3 days. Stimulant-like effects (energy, focus) typically felt day one. Full weight loss effects over 2-4 weeks at steady state.
Can I take tesofensine with coffee?
Yes, but reduce caffeine by 50%. Tesofensine amplifies stimulant effects through norepinephrine and dopamine — jitteriness and elevated heart rate are common if you don't adjust.
Is tesofensine better than semaglutide for weight loss?
Different mechanisms, hard to compare directly. Tesofensine works via monoamine reuptake (appetite + energy), semaglutide via GLP-1 (satiety + gastric emptying). Some users stack both. See our tesofensine weight loss guide for a detailed comparison.
What happens if I miss a dose?
Take it if still morning. Skip if afternoon/evening — the long half-life means late dosing causes insomnia. Resume next morning.
References
| Citation |
Topic |
PMID |
| Astrup et al., The Lancet (2008) |
Phase II RCT: 0.5mg = 11.3% weight loss in 24 weeks |
18579710 |
| Sjödin et al., Int J Obesity (2010) |
Energy expenditure and appetite effects of tesofensine |
21414090 |
| Hauser et al., Neurology (2007) |
Tesofensine safety data from Parkinson's disease trials |
18202642 |
| Appel et al., Drugs of Today (2014) |
Tesofensine development history and pharmacology |
23741593 |
| Gilbert et al., Obesity (2012) |
Tesofensine effects on appetite sensations |
19169362 |
For educational and research purposes only. This is not medical advice. Tesofensine is not FDA-approved for any indication.