MK-677 (ibutamoren) is a non-peptide growth hormone secretagogue that mimics ghrelin to stimulate natural GH release. Unlike most compounds in the peptide space, MK-677 is orally bioavailable — no injections required — and has human clinical data spanning up to 2 years of continuous use.
Research-context information only.MK-677 (ibutamoren) is a research peptide. Protocols, doses, and reactions reported below come from published research and self-reported community sources. This article reports what has been documented, not what should be done. Consult a licensed physician for personal medical decisions.
Most people reach for MK-677 expecting muscle growth. The clinical data tells a more nuanced story. This guide ranks every researched benefit by evidence quality — strongest first, weakest last.
This is not medical advice. MK-677 is not FDA-approved for any indication and is sold as a research chemical.
How MK-677 Works
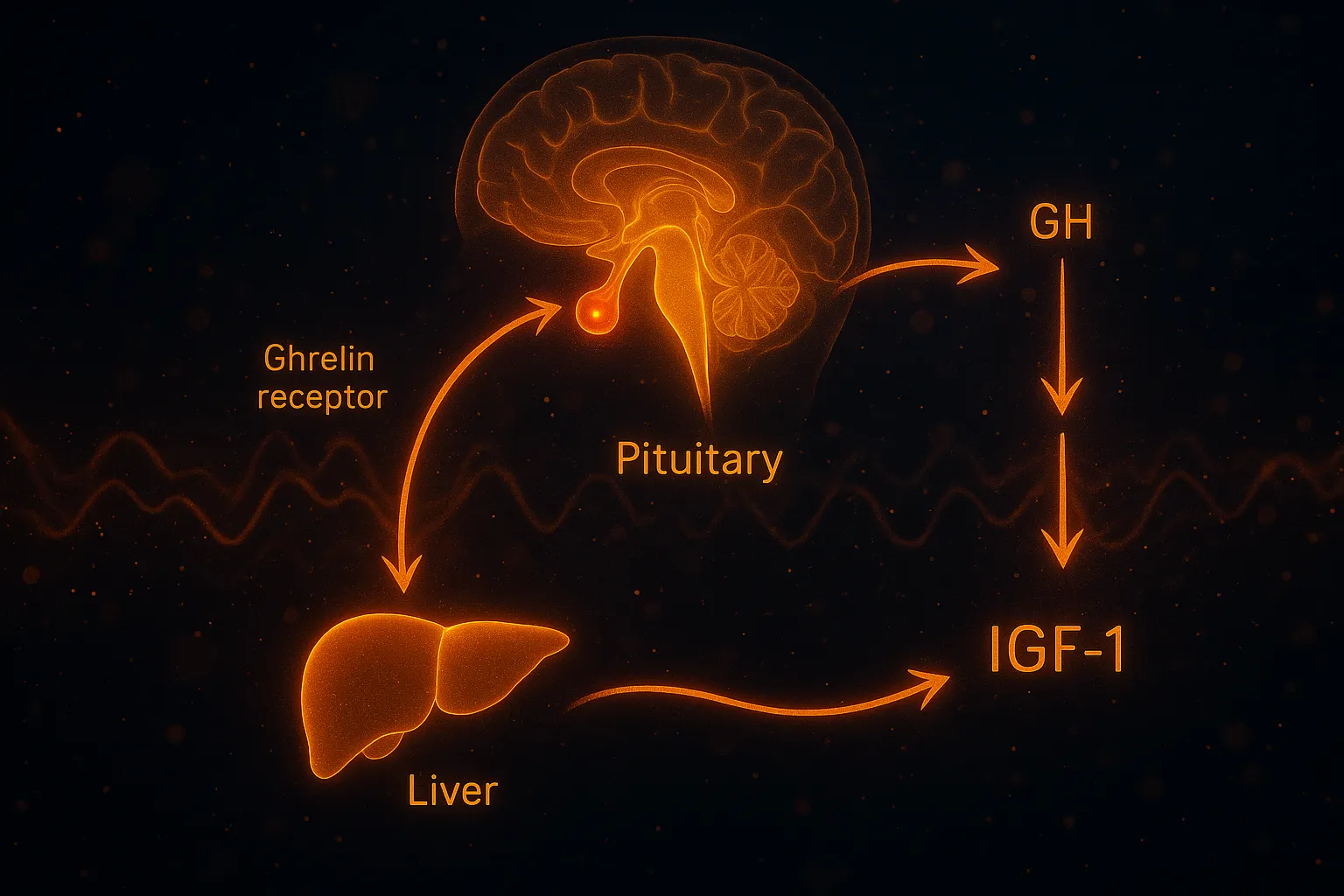
MK-677 binds to the ghrelin receptor (GHS-R1a) on pituitary somatotrophs, mimicking the hunger hormone ghrelin. This triggers a signaling cascade that results in growth hormone release — but unlike exogenous GH injections, MK-677 preserves the body's natural pulsatile GH pattern (Murphy et al., 1998).
The downstream effects flow through two pathways. GH acts directly on tissues (lipolysis, protein synthesis), and it also stimulates IGF-1 production in the liver. IGF-1 mediates most of the anabolic and tissue-repair effects attributed to growth hormone (Nass et al., 2008).
Critically, MK-677 does not suppress endogenous GH production through negative feedback — a key safety distinction from exogenous GH. For full dosing protocols, see our MK-677 Dosing Guide.
1. Sleep Quality Improvement
Evidence: Human — Controlled Trial
This is MK-677's most directly measured benefit. Copinschi et al. (1997) used polysomnography (objective sleep measurement) to evaluate MK-677's effect on sleep architecture in both young (18-30) and older (65-71) adults (PMID 9349662).
Results in young subjects at 25mg bedtime dosing:
Stage IV (deep) sleep duration increased by approximately 50%
REM sleep increased by over 20%
Deviations from normal sleep patterns dropped from 42% to 8%
Older adults showed a nearly 50% increase in REM sleep and decreased REM latency (fell into REM faster). The researchers concluded that MK-677 may simultaneously improve sleep quality and correct age-related GH decline.
Why this matters: Deep sleep is when the body performs most tissue repair, memory consolidation, and natural GH release. Improving Stage IV sleep has cascading effects on recovery, cognition, and metabolic health. This is why bedtime dosing is the standard protocol.
2. GH and IGF-1 Elevation
Evidence: Human — Multiple Controlled Trials
The core pharmacological effect of MK-677. Nass et al. (2008) demonstrated in a 2-year randomized controlled trial that 25mg daily MK-677 restored GH and IGF-1 levels in healthy older adults to the range seen in young adults — and maintained these levels for the full study duration (PMID 18981485).
Murphy et al. (1998) confirmed in a separate trial that MK-677 significantly increased GH and IGF-1 in healthy volunteers and reversed diet-induced nitrogen wasting (catabolism), suggesting a protein-sparing, anabolic effect (PMID 9467534).
IGF-1 elevation occurs within days of starting treatment and persists throughout use (Copinschi et al., 1996).
Why this matters: GH and IGF-1 decline progressively from young adulthood onward — a process called somatopause. Restoring these levels to the young-adult range is the mechanistic basis for most of MK-677's downstream benefits (body composition, sleep, bone, recovery).
3. Lean Body Mass (Fat-Free Mass)
Evidence: Human — 2-Year RCT
The Nass 2008 study found that MK-677 recipients gained significant fat-free mass over 12 months while the placebo group lost fat-free mass (PMID 18981485). This is consistent with GH's known protein-synthetic and anti-catabolic effects.
Important caveat: the increase in fat-free mass did not translate to measurable improvements in strength or physical function in this elderly population. This suggests the lean mass gains may partly reflect water retention in muscle tissue (a known effect of GH elevation) rather than purely contractile muscle fiber growth.
Why this matters: MK-677 reliably increases lean body mass — the number on a DEXA scan goes up. Whether this represents functional muscle gain versus GH-mediated water retention in muscle remains an open question. For younger, resistance-trained individuals, the anabolic signal combined with training stimulus may yield more functional results than seen in sedentary elderly subjects.
Ready to buy? See our MK-677 buying guide for format comparison, COA verification, and pricing.
10mg · sold research-use-only · we may earn a commission
4. Anti-Catabolic Effects (Muscle Preservation)
Evidence: Human — Controlled Trial
Murphy et al. (1998) specifically tested MK-677's ability to counteract muscle breakdown during caloric restriction. Subjects on a calorie-restricted diet who received MK-677 showed reversal of diet-induced nitrogen wasting — meaning the peptide preserved muscle protein despite the catabolic environment (PMID 9467534).
This is a distinct benefit from muscle growth. Even if MK-677 doesn't dramatically build new muscle, it may protect existing muscle during dieting, illness, or periods of reduced activity.
Why this matters: Muscle loss during caloric deficit is one of the biggest challenges in body recomposition. An oral compound that preserves lean tissue while dieting has practical value beyond what the muscle growth data alone suggests.
5. Bone Turnover and Density
Evidence: Human — Multiple Trials
MK-677 increases markers of both bone formation and resorption — a process called "bone remodeling." Svensson et al. (1998) demonstrated this in obese young males over 2 months (PMID 9661080).
In postmenopausal women with osteoporosis, Murphy et al. (2001) found that MK-677 combined with alendronate increased femoral neck BMD by 4.2% versus 2.5% with alendronate alone (PMID 11238495).
The Nass 2-year study also noted bone mineral density changes consistent with increased bone remodeling in MK-677 recipients.
Why this matters: Bone density benefits require long time horizons (6-12+ months). The initial increase in bone turnover markers is not immediately beneficial — both formation and resorption increase. Over time, the net effect appears positive, particularly when combined with anti-resorptive agents. This is relevant for aging populations and those at risk for osteoporosis.
6. Appetite Stimulation
Evidence: Human — Multiple Trials, Consistent Finding
MK-677 is a ghrelin mimetic — increased appetite is not a side effect, it's a primary pharmacological action. It occurs in the majority of users, typically within the first week.
For most people seeking fat loss or body recomposition, this is a disadvantage. But for populations struggling with insufficient caloric intake — the elderly, those recovering from illness, or individuals with suppressed appetite from other medications — appetite stimulation can be clinically useful.
Chapman et al. (1996) documented the appetite-stimulating properties as part of MK-677's ghrelin receptor activation profile (PMID 8954023).
Why this matters: Context determines whether this is a benefit or a drawback. For hardgainers and recovery populations, it's advantageous. For weight loss goals, it requires management (bedtime dosing helps mitigate daytime hunger).
7. No Suppression of Natural GH Production
Evidence: Human — 2-Year Data
Unlike exogenous growth hormone injections, MK-677 stimulates the body's own GH release mechanism rather than replacing it. The 2-year Nass study confirmed that MK-677 did not suppress endogenous GH production and that GH levels returned to baseline within 2-4 weeks of discontinuation (PMID 18981485).
This is a structural advantage of the ghrelin-mimetic mechanism — it works with the body's feedback systems rather than overriding them.
Why this matters: One of the biggest concerns with exogenous GH is pituitary suppression. MK-677 avoids this entirely. Cycling on and off doesn't carry the recovery burden that exogenous GH does.
Most clinical benefits were observed at 25mg daily taken at bedtime. Community protocols typically start at 10mg and titrate to 20-25mg based on tolerance.
For complete dosing protocols, cycling, and stacking options, see the MK-677 Dosing Guide.
Who Should Consider MK-677
Based on the evidence, MK-677 is most relevant for:
Sleep optimization — those seeking deeper sleep without sedatives or tolerance buildup
Muscle preservation during cuts — the anti-catabolic data supports use during caloric deficit
Injection-averse individuals — oral dosing eliminates the barrier of daily subcutaneous injections
GH peptide stacking — MK-677 provides baseline oral GH elevation that complements injectable peptides like ipamorelin or CJC-1295
MK-677 may be less suitable for those with pre-diabetic markers (due to insulin resistance effects), those prioritizing appetite suppression for weight loss, or competitive athletes (WADA prohibited).
Bac Water Made for Peptides
Don't risk a $300 peptide on generic bac water.
Most cloudy reconstitutions trace back to one thing — and it isn't the peptide. Sterile, non-pyrogenic, 0.9% benzyl alcohol — formulated for peptide reconstitution, not repackaged from generic stock.
✓ 0.9% benzyl alcohol✓ Made for peptides✓ 30 mL multi-dose
30ml from $18.75 · Ships fast · Code thepeptidecatalog
Frequently Asked Questions
What is the most proven benefit of MK-677?
Sleep quality improvement has the strongest direct evidence. A controlled study (Copinschi et al., 1997) showed MK-677 increased Stage IV deep sleep by 50% and REM sleep by 20% in young subjects, with similar improvements in older adults. This effect was consistent and directly measured via polysomnography.
Does MK-677 build muscle?
MK-677 increases fat-free mass (lean body mass) — the 2-year Nass study showed significant gains. However, this did not translate to measurable strength improvements in that trial. The increase in lean mass is likely driven by GH-mediated protein synthesis and water retention in muscle tissue.
Is MK-677 better than injectable GH peptides?
MK-677's advantage is oral dosing — no injections required. Its GH elevation is modest compared to injectable peptides like ipamorelin or GHRP-2, but it maintains natural pulsatile release patterns. For pure GH output, injectables are stronger. For convenience and compliance, MK-677 wins.
How long does MK-677 take to show benefits?
Sleep improvements appear within the first week. IGF-1 elevation occurs within days and stabilizes by week 2-4. Body composition changes (fat loss, lean mass) typically become noticeable at 8-12 weeks. Bone density changes require 6-12 months of use.
Does MK-677 cause insulin resistance?
Yes — mild, reversible insulin resistance is a documented side effect. Fasting glucose and HbA1c may increase during use. This reverses after discontinuation. Monitoring blood sugar is recommended, especially for those with pre-diabetic markers.
Research Supplies for MK-677 (Ibutamoren)
Hand-picked storage, injection, and recovery supplies paired with MK-677 (Ibutamoren) protocols.
For educational and research purposes only. This is not medical advice. MK-677 is not FDA-approved for any indication and is sold as a research chemical.