GHRP-2 and GHRP-6 are the two most commonly compared growth hormone releasing peptides. They share a receptor target, a mechanism of action, and a similar dosing range — but they produce meaningfully different experiences, particularly when it comes to appetite stimulation and research applications.
This comparison breaks down exactly how these two peptides differ based on the clinical literature. If you're new to the GHRP family, start with our GHRH vs GHRP mechanistic breakdown for the foundational science.
Overview
Both GHRP-2 (pralmorelin/KP-102) and GHRP-6 are synthetic hexapeptides that stimulate growth hormone release from the anterior pituitary through the growth hormone secretagogue receptor type 1a (GHSR-1a) — the ghrelin receptor (Howard et al., 1996).
They were developed as part of Cyril Bowers' pioneering work on GH secretagogues in the 1980s-90s (Bowers, 1998), and both predated the discovery of ghrelin itself (Kojima et al., 1999). GHRP-6 came first chronologically; GHRP-2 was developed as an optimized analog with a modified amino acid sequence.
GHRP-2: D-Ala-D-βNal-Ala-Trp-D-Phe-Lys-NH₂
GHRP-6: His-D-Trp-Ala-Trp-D-Phe-Lys-NH₂
For the full individual profiles, see our GHRP-2 Dosing Guide and GHRP-6 Complete Guide. For a deeper look at each peptide's effects, see the GHRP-2 Benefits Guide and GHRP-6 Benefits Guide. For a broader comparison including ipamorelin, see our three-way GHRP comparison.
Mechanism Comparison
Shared Pathway
Both peptides activate GHSR-1a on pituitary somatotrophs, triggering:
GHSR-1a → Gq/11 → PLC → IP₃ + DAG → intracellular Ca²⁺ release → PKC activation → Ca²⁺ influx → GH vesicle exocytosis
This is fundamentally different from how GHRH analogs (CJC-1295, Sermorelin) work (GHRHR → Gs → cAMP → PKA), which is why combining either GHRP with a GHRH analog produces synergistic GH release (Veldhuis et al., 2009).
Both peptides also act centrally — stimulating hypothalamic GHRH neurons and antagonizing somatostatin tone, amplifying GH release beyond what pituitary-level action alone would produce.
Where They Diverge
Despite sharing the same receptor, GHRP-2 and GHRP-6 differ in their downstream signaling emphasis, particularly in hypothalamic circuits:
- GHRP-6 more potently engages NPY/AgRP orexigenic neurons in the arcuate nucleus, producing significantly stronger appetite stimulation
- GHRP-2 appears to engage these appetite circuits less intensely while maintaining comparable somatotroph-level GH release
The structural difference — GHRP-2's D-βNal at position 2 vs GHRP-6's D-Trp — likely influences binding kinetics and the balance of signaling outputs at GHSR-1a. The receptor itself couples to multiple G proteins (Gq/11, Gi/o, G12/13, and β-arrestin), and different agonists can bias signaling toward different pathways (Overlapping binding site study, 2008).
GH Release Potency
Head-to-Head Data
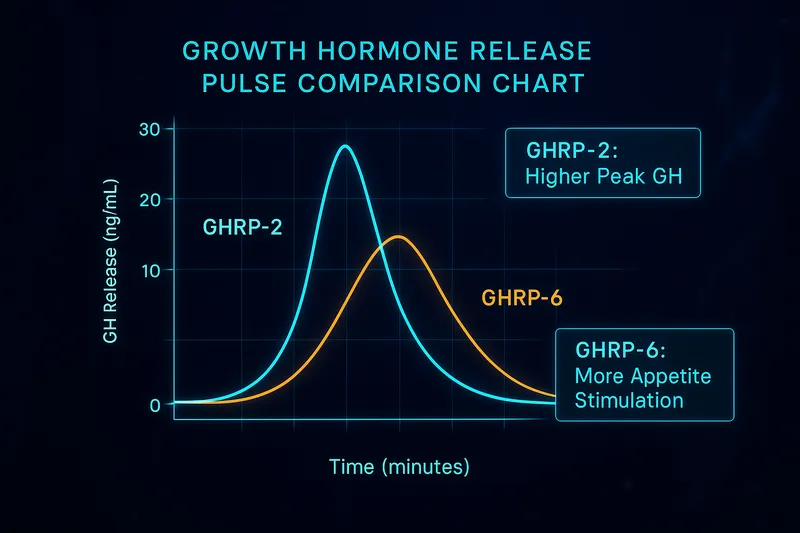
At equivalent doses (1-2 mcg/kg), both peptides produce comparable GH release:
| Metric |
GHRP-2 |
GHRP-6 |
| Peak GH |
30-80 ng/mL |
30-90 ng/mL |
| Time to Peak |
30-60 min |
30-60 min |
| Duration |
2-3 hours |
2-3 hours |
| Dose-Response Plateau |
~2-3 mcg/kg |
~2-3 mcg/kg |
GHRP-6 may produce slightly higher peak values in some studies, but the difference is modest and varies with population, body composition, and sex steroid status. Neither peptide consistently outperforms the other in raw GH output.
Both peptides show similar response attenuation with continuous daily use, and both produce the same magnitude of synergy when combined with GHRH analogs (Veldhuis et al., 2008).
Context: Where Do They Rank?
Within the GHRP family:
- Hexarelin — Strongest GH release (but most side effects). See our Hexarelin deep dive
- GHRP-2 / GHRP-6 — Strong GH release, mid-range side effects
- Ipamorelin — Moderate GH release, minimal side effects
The practical GH release difference between GHRP-2 and GHRP-6 is not the deciding factor between them. Other characteristics matter more.
Ready to buy? Compare verified vendors on our best GHRP-2 sources page, or browse all coupon codes for up to 50% off.
Side Effect Profiles
This is where the two peptides diverge most meaningfully.
Cortisol
Both peptides stimulate the HPA axis through CRF-mediated ACTH release (ACTH releasing activity of KP-102, 2005):
|
GHRP-2 |
GHRP-6 |
| ACTH stimulation |
Moderate |
Moderate |
| Cortisol elevation |
Moderate, transient |
Moderate, transient |
| Clinical relevance |
Used as HPA axis test |
Comparable |
Ghigo et al. found comparable ACTH and cortisol responses between GHRP-2 and hexarelin (Ghigo et al., 1997). GHRP-6 shows a similar profile. The cortisol response is not a meaningful differentiator between these two peptides.
The GHRP-2 stimulation test has been validated as an alternative to the insulin tolerance test for HPA axis evaluation (GHRP-2 vs ITT for HPA assessment, 2018).
Prolactin
Both peptides cause modest, dose-dependent prolactin elevation:
|
GHRP-2 |
GHRP-6 |
| Prolactin increase |
Mild-moderate |
Mild-moderate |
| Duration |
Transient (2-3 hr) |
Transient (2-3 hr) |
| Dose-dependence |
Yes |
Yes |
Again, not a significant differentiator. Both are less prolactin-stimulating than hexarelin at high doses.
Hunger — The Key Difference
This is the decisive distinction:
|
GHRP-2 |
GHRP-6 |
| Appetite stimulation |
Mild-moderate |
Intense |
| Onset |
~20-30 min |
~20 min |
| Duration |
20-40 min |
30-60 min |
| Subjective intensity |
Noticeable |
Hard to ignore |
GHRP-6 produces significantly stronger hunger signals than GHRP-2. This is the single most important practical difference between the two peptides and the primary factor in choosing between them.
The orexigenic effect is mediated through GHSR-1a activation of NPY/AgRP neurons in the hypothalamus, with downstream engagement of reward circuits in the ventral tegmental area (Ghrelin signaling in VTA, 2015).
Dosing Comparison
| Parameter |
GHRP-2 |
GHRP-6 |
| Standard dose |
100-200 mcg (1-2 mcg/kg) |
100-200 mcg (1-2 mcg/kg) |
| Upper range |
300 mcg |
300 mcg |
| Frequency |
2-3x daily |
2-3x daily |
| Administration |
SC injection, fasted |
SC injection, fasted |
| Timing |
30-60 min before meals or 2+ hr after |
30-60 min before meals or 2+ hr after |
| Half-life |
~15-30 min |
~15-30 min |
| Desensitization risk |
Yes, with continuous use |
Yes, with continuous use |
Dosing is essentially identical between the two peptides. The pharmacokinetics are comparable — rapid absorption, short half-life, similar GH peak timing.
GHRP-2 has more clinical dosing data due to its use as a diagnostic agent in Japan (Simple diagnostic test using GHRP-2, 2007), while GHRP-6 has detailed pharmacokinetic characterization from a healthy volunteer study (PK study of GHRP-6, 2012).
Who Should Use Which?
Choose GHRP-2 if:
- You want GH stimulation without intense hunger — GHRP-2's milder appetite effect makes it more practical for those who don't want to deal with powerful hunger surges
- You're combining with a GHRH analog — Both peptides synergize equally well with CJC-1295 or Sermorelin, but GHRP-2's lower appetite impact makes the combination more comfortable
- You're lean and trying to stay lean — Intense hunger can sabotage body composition goals
- You want the most studied diagnostic variant — GHRP-2 has more clinical validation as a pituitary function test
Choose GHRP-6 if:
- Appetite stimulation is a feature, not a bug — Recovery from illness, post-surgery, cachexia, or deliberate caloric surplus goals benefit from GHRP-6's orexigenic effect
- You're interested in cytoprotective applications — GHRP-6 has a more extensive literature on cardioprotection, neuroprotection, and tissue protection (GHRP-6 cardioprotection, 2024)
- You're underweight or struggling to eat enough — The appetite boost can be therapeutic
- You want the historical "first" GHRP — GHRP-6 has the longest research track record in the family
Choose Neither (Consider Alternatives) if:
- You want minimal side effects → Ipamorelin (most selective GHSR-1a agonist)
- You want maximum GH potency → Hexarelin (strongest GHRP, but highest cortisol/prolactin). See our Hexarelin guide
- You want sustained GH elevation → CJC-1295 with DAC (GHRH analog, different mechanism entirely). See CJC-1295 vs Sermorelin
Stacking Considerations
Both GHRP-2 and GHRP-6 stack identically well with GHRH analogs — the synergy is a receptor-level phenomenon, not specific to one GHRP over another.
GHRP-2 + CJC-1295
- Synergistic GH release through dual-pathway convergence
- Moderate appetite stimulation
- Good for those prioritizing GH output with manageable side effects
- The most commonly discussed "clean" GHRP + GHRH stack
GHRP-6 + CJC-1295
- Equal GH synergy to the GHRP-2 combination
- Significantly more appetite stimulation
- Better for recovery/surplus phases where eating more is the goal
- More cytoprotective research backing
Can You Stack GHRP-2 + GHRP-6?
There's no clinical data specifically examining GHRP-2 + GHRP-6 co-administration. Since they activate the same receptor (GHSR-1a), combining them wouldn't produce the same synergy as pairing either with a GHRH analog (which uses a different receptor). They would compete for GHSR-1a binding rather than activate complementary pathways.
The evidence-based stacking principle: GHRP + GHRH = synergy. GHRP + GHRP = competition.
For comprehensive stacking strategies, see our Peptide Stacking Guide.
Research Applications: Where Each Peptide Shines
GHRP-2 in Clinical Diagnostics
GHRP-2 has carved out a unique niche as a diagnostic tool for growth hormone deficiency. It is approved in Japan (as pralmorelin) for the GHRP-2 stimulation test, which assesses pituitary GH reserve capacity (Clinical usefulness of GHRP-2 test, 2022). The test has also been validated for evaluating HPA axis function, potentially replacing the insulin tolerance test in certain contexts (GHRP-2 vs ITT, 2018).
GHRP-2 has also been studied for its ability to stimulate GH in patients with mutated GHRH receptors — demonstrating that GHSR-1a provides an independent rescue pathway for GH release even when the GHRH axis is compromised (Maheshwari et al., 2002).
Additionally, intranasal GHRP-2 has been explored as a long-term therapeutic option, with a one-year intranasal application study showing improvements in body weight and hypoglycemia in a severely malnourished patient (Intranasal GHRP-2, 2015).
GHRP-6 in Cytoprotection and Tissue Repair
GHRP-6's research literature extends significantly beyond GH release into tissue protection and repair:
- Stroke therapy: A Phase I/II clinical trial examined GHRP-6 combined with recombinant EGF for acute ischemic stroke — one of the few GHS compounds to reach clinical trials for a non-endocrine indication (Berlanga-Acosta et al., 2024)
- Lung injury: GHRP-6 ameliorates acute lung injury and prevents its progression to interstitial fibrosis in preclinical models (GHRP-6 in lung injury, 2025)
- Organ failure prevention: GHRP-6 has been investigated for multiple organ failure prevention in critical illness (Berlanga-Acosta et al., 2006)
- Cardiac protection: The peptide protects against doxorubicin-induced cardiotoxicity through prosurvival pathway activation (GHRP-6 cardioprotection, 2024)
These cytoprotective effects appear to involve GHSR-1a-mediated anti-inflammatory, anti-apoptotic, and antioxidant signaling — potentially independent of GH release itself.
The Takeaway
GHRP-2 = more clinical validation for endocrine diagnostics and GH axis evaluation.
GHRP-6 = more preclinical and early-clinical data on tissue protection and repair beyond GH release.
Frequently Asked Questions
Is GHRP-2 or GHRP-6 better for building muscle?
Neither peptide has been directly studied for muscle building in controlled clinical trials. Both stimulate comparable GH release, which supports protein synthesis and recovery. The choice between them for this goal comes down to whether you want the appetite boost (GHRP-6) or prefer to avoid it (GHRP-2).
Can I switch between GHRP-2 and GHRP-6?
They share the same receptor, so switching is straightforward — no washout period is needed. Some researchers alternate between them to leverage GHRP-6's appetite effects during surplus phases and GHRP-2's cleaner profile during other phases.
Which GHRP has the fewest side effects overall?
Neither GHRP-2 nor GHRP-6 — that distinction goes to ipamorelin, which produces minimal cortisol, prolactin, and appetite effects. See our three-way comparison.
Do GHRP-2 and GHRP-6 affect sleep?
Both peptides, when administered before bed, can amplify the natural nocturnal GH surge. Neither has been associated with sleep disruption in the clinical literature. The bedtime dose is one of the most commonly used timing strategies.
Verdict
GHRP-2 and GHRP-6 are more similar than different. They share the same receptor, the same signaling pathway, comparable GH release potency, similar dosing protocols, and overlapping side effect profiles (cortisol, prolactin).
The deciding factor is hunger.
- If intense appetite stimulation is unwanted → GHRP-2
- If appetite stimulation is beneficial → GHRP-6
Everything else — GH potency, cortisol impact, prolactin elevation, synergy with GHRH analogs, dosing — is essentially equivalent between the two.

For most research contexts where GH stimulation is the primary goal and hunger is an unwanted side effect, GHRP-2 is the more practical choice. For contexts where appetite support, cytoprotection, or recovery from illness are relevant, GHRP-6's additional properties provide meaningful advantages.
And if side effects are the primary concern over raw GH potency, neither GHRP-2 nor GHRP-6 is optimal — ipamorelin offers the cleanest side effect profile in the GHRP family, albeit with somewhat less GH output. See our GHRP comparison guide for the full three-way analysis.
References
- Bowers CY. Growth hormone-releasing peptide (GHRP). Cell Mol Life Sci. 1998;54(12):1316-29. PMID: 9893708
- Howard AD, et al. A receptor in pituitary and hypothalamus that functions in growth hormone release. Science. 1996;273(5277):974-7. PMID: 8688086
- Kojima M, et al. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402(6762):656-60. PMID: 10604470
- Bowers CY. Unnatural growth hormone-releasing peptide begets natural ghrelin. J Clin Endocrinol Metab. 2001;86(4):1464-9. PMID: 11297568
- Veldhuis JD, et al. Determinants of GH-releasing hormone and GH-releasing peptide synergy in men. Am J Physiol. 2009;296(4):E1085-92. PMID: 19240251
- Veldhuis JD, et al. Gonadal status and body mass index jointly determine GHRH/GHRP synergy. J Clin Endocrinol Metab. 2008;93(11):4221-9. PMID: 18073313
- Ghigo E, et al. Effects of GHRP-2 and hexarelin on GH, prolactin, ACTH and cortisol levels in man. Eur J Endocrinol. 1997;136(1):87-92. PMID: 9285939
- ACTH releasing activity of KP-102 (GHRP-2) mediated by CRF release. J Pharmacol Sci. 2005;97(1):67-73. PMID: 15645295
- Evaluation of HPA axis by the GHRP2 test vs ITT. J Endocr Soc. 2018;2(12):1457-67. PMID: 30324179
- GHRP-6 prevents doxorubicin-induced myocardial damage. Biomed Pharmacother. 2024;170:116043. PMID: 38873418
- Simple diagnostic test using GH-releasing peptide-2. Eur J Endocrinol. 2007;157(1):19-27. PMID: 17609397
- PK study of GHRP-6 in healthy volunteers. Eur J Pharm Sci. 2012;48(1-2):40-6. PMID: 23099431
- Ghrelin signaling in VTA mediates reward-based feeding. Neuropsychopharmacology. 2015;40(9):2168-77. PMID: 25967263
- Overlapping binding site for agonists and allosteric modulators on GHSR. Mol Pharmacol. 2008;75(1):44-59. PMID: 18923064
- Teichman SL, et al. Prolonged stimulation of GH and IGF-I by CJC-1295. J Clin Endocrinol Metab. 2006;91(3):799-805. PMID: 16352683
This article is for educational and informational purposes only. It is not medical advice. GHRP-2 and GHRP-6 are research compounds — consult a qualified healthcare provider before considering any peptide protocol.