GHRP-6 (Growth Hormone Releasing Peptide-6) is one of the original synthetic growth hormone secretagogues and remains one of the most researched peptides in the GHS family. It's known for two things: potent GH release from the anterior pituitary and significant appetite stimulation — a direct consequence of its action on the ghrelin receptor.
First synthesized in the early 1980s as part of Cyril Bowers' groundbreaking work on growth hormone releasing peptides (Bowers, 1998), GHRP-6 predates the discovery of ghrelin itself and played a key role in identifying the GHS receptor system that would later be recognized as the ghrelin signaling axis (Bowers, 2001).
This guide covers GHRP-6 comprehensively: its mechanism, what makes it different from GHRP-2, dosing protocols from clinical research, benefits beyond GH release, side effects, and practical considerations. For the foundational science on how GHRPs differ from GHRH analogs, see our GHRH vs GHRP mechanistic breakdown.
What Is GHRP-6?
GHRP-6 is a synthetic hexapeptide with the sequence His-D-Trp-Ala-Trp-D-Phe-Lys-NH₂. It was one of the first compounds developed to stimulate GH release through a pathway independent of GHRH — what would later be identified as the growth hormone secretagogue receptor (GHSR-1a) or ghrelin receptor.
Key characteristics:
- Molecular weight: ~873 Da
- Half-life: Approximately 15-30 minutes
- Route: Subcutaneous injection (primary research route)
- GH release onset: 15-30 minutes post-administration
- Peak GH levels: 30-60 minutes post-injection
- Distinguishing feature: Strong appetite stimulation via ghrelin receptor activation
GHRP-6 was instrumental in the discovery of the entire ghrelin system. The existence of synthetic peptides that released GH through an unknown receptor led researchers to clone GHSR-1a in 1996 (Howard et al., 1996), and subsequently to identify ghrelin as its endogenous ligand in 1999 (Kojima et al., 1999). As Bowers noted, the "unnatural" peptide led directly to the discovery of the "natural" hormone (Bowers, 2001).
For how GHRP-6 compares directly to GHRP-2 and ipamorelin, see our three-way GHRP comparison.
Mechanism of Action
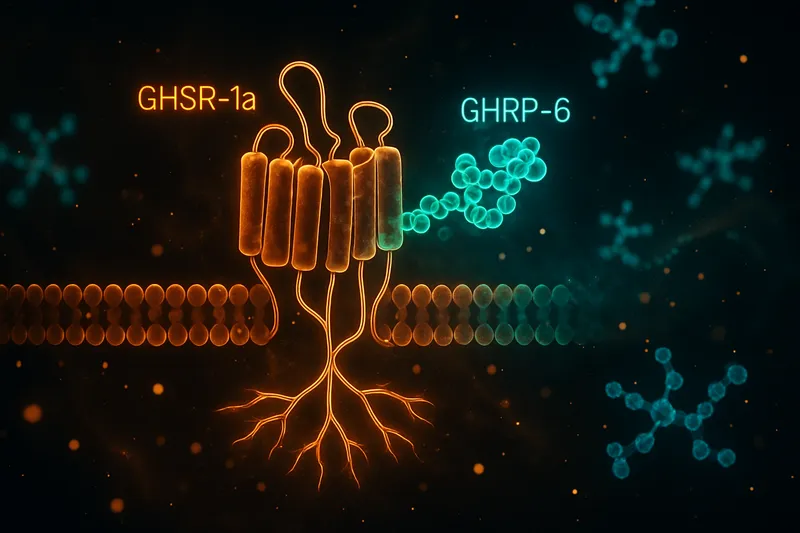
GHRP-6 acts primarily through the growth hormone secretagogue receptor type 1a (GHSR-1a), a G protein-coupled receptor expressed in the pituitary gland, hypothalamus, and numerous peripheral tissues.
Pituitary GH Release
At the pituitary level, GHRP-6 binding to GHSR-1a on somatotroph cells triggers:
- Gq/11 protein activation → Phospholipase C (PLC) stimulation
- IP₃ and DAG generation → Intracellular calcium mobilization from ER stores
- Protein Kinase C (PKC) activation → Modulation of voltage-gated calcium channels
- Calcium influx → GH vesicle exocytosis and release
This is the same fundamental signaling cascade used by GHRP-2 and all GHSR-1a agonists. The critical distinction from GHRH is the receptor and second messenger system: GHRH activates GHRHR → Gs → cAMP → PKA, while GHRPs activate GHSR-1a → Gq → PLC → PKC. This pathway divergence is why combining GHRP-6 with a GHRH analog produces synergistic GH release — the two pathways converge on calcium-dependent vesicle fusion through different routes. Our GHRH vs GHRP article explains these dual pathways in depth.
Hypothalamic Actions
GHRP-6 also acts centrally within the hypothalamus:
- Stimulates GHRH neurons in the arcuate nucleus, increasing endogenous GHRH tone
- Antagonizes somatostatin signaling, reducing the inhibitory brake on GH release
- Activates NPY/AgRP neurons in the arcuate nucleus — this is the primary driver of GHRP-6's pronounced appetite-stimulating effects
This dual pituitary + hypothalamic action makes GHRP-6 a more potent GH secretagogue than its mechanism at either site alone would predict.
Ghrelin Mimicry and Appetite
GHRP-6 is a particularly strong ghrelin mimetic when it comes to orexigenic (appetite-stimulating) effects. While all GHRPs activate GHSR-1a, GHRP-6 appears to engage the hunger signaling components of ghrelin biology more robustly than GHRP-2 or ipamorelin.
The mechanism involves:
This appetite effect is a feature for some applications (recovery from illness, cancer cachexia) and a side effect for others.
Key Difference from GHRP-2
While GHRP-6 and GHRP-2 share the same receptor target (GHSR-1a) and the same fundamental signaling pathway, they differ in several clinically meaningful ways:
Appetite Stimulation
GHRP-6 produces markedly stronger hunger than GHRP-2. This is the single most obvious difference users of both peptides report, and it's supported by the preclinical literature. GHRP-6's activation of hypothalamic appetite circuits appears more pronounced, potentially due to differences in receptor binding kinetics or engagement of accessory signaling pathways.
GH Release Potency
Both peptides produce robust GH release at equivalent doses. GHRP-6 may produce slightly higher peak GH values in some studies, though this varies across populations and protocols. The difference is modest compared to the difference in appetite effects.
Side Effect Burden
GHRP-6 tends to cause:
- More pronounced appetite stimulation (sometimes intense hunger within 20 minutes)
- Comparable cortisol elevation to GHRP-2
- Similar prolactin stimulation
Cytoprotective Research
GHRP-6 has a more developed literature on cytoprotective and cardioprotective effects than GHRP-2, with extensive research from Cuban and international groups on its tissue-protective properties (covered in the Benefits section below).
GHRP-6 Dosing Protocols
Dose Range
Clinical and preclinical research on GHRP-6 has used a range of doses:
- 1 mcg/kg (~100 mcg): Standard dose used in many clinical studies. Produces robust GH release with moderate side effects.
- 2 mcg/kg (~150-200 mcg): Higher dose used in some protocols. Greater GH output but proportionally more appetite stimulation and cortisol elevation.
- 100-300 mcg per injection: The practical range, with most research centering on 100-200 mcg.
A pharmacokinetic study in nine healthy male volunteers characterized GHRP-6's absorption and distribution profile, confirming rapid absorption after subcutaneous injection with peak plasma concentrations within minutes (PK study of GHRP-6, 2012).
Timing
Like all GHRPs, GHRP-6 should be administered on an empty stomach for optimal GH response:
- Fasted state: 30-60 minutes before food, or 2+ hours after eating
- Why: Elevated glucose, insulin, and free fatty acids suppress the GH response to GHSR-1a activation
- Note: Given GHRP-6's strong appetite stimulation, timing it before a planned meal can be practical — the hunger hits approximately 20-30 minutes post-injection
Frequency
- 2-3 times daily in multi-dose protocols
- Common timing: Morning fasted, pre-workout (if training fasted), and before bed
- Minimum spacing: 3+ hours between doses to allow GHSR-1a resensitization
Desensitization
Like GHRP-2, continuous daily GHRP-6 use can lead to receptor desensitization and attenuated GH response over time. Cycling strategies (e.g., 5 on / 2 off, or periodic breaks) may help maintain receptor sensitivity.
Benefits of GHRP-6
1. Pulsatile GH Release
The primary benefit of GHRP-6 is stimulating endogenous GH release in a pulsatile pattern that approximates natural physiology. Unlike exogenous GH injections (which create a flat, non-physiologic pharmacokinetic profile), GHRP-6 triggers the pituitary to release its own stored GH in bursts.
This pulsatile release pattern is important because GH's downstream effects — including IGF-1 production, lipolysis, and protein synthesis — are partially dependent on the pulsatile signal rather than continuous GH exposure.
2. Appetite Stimulation for Recovery
GHRP-6's potent orexigenic effects make it particularly relevant in research on:
- Cancer cachexia — Loss of appetite and muscle wasting in cancer patients
- Chemotherapy-associated anorexia — Similar to findings with GHRP-2 (GHRP-2 reverses chemotherapy anorexia, 2008)
- Recovery from illness or surgery — When increased caloric intake is beneficial
- Underweight conditions — Where appetite stimulation supports weight gain
The gastrointestinal effects of GHRP-6 have been characterized, including its stimulation of upper GI contractile activity and food intake (GHRP-2 GI effects in dogs, 2009).
3. Cytoprotective and Cardioprotective Effects
GHRP-6 has a substantial body of research on tissue-protective effects that extend beyond GH release:
Cardioprotection:
Neuroprotection:
Cell Turnover:
- GHRP-6 has differential beneficial effects on cell turnover in the pituitary, hypothalamus, and heart — distinct from insulin's effects in the same tissues (GHRP-6 cell turnover effects, 2011)
4. Synergistic GH Release with GHRH
Like all GHRPs, GHRP-6 produces synergistic GH output when combined with GHRH analogs. This synergy has been extensively documented by Veldhuis et al. and is the scientific basis for GHRP + GHRH stacking protocols (Veldhuis et al., 2009).
For practical stacking strategies, see our Peptide Stacking Guide.
Side Effects
Appetite Stimulation (The Dominant Side Effect)
GHRP-6's most prominent side effect is intense hunger, typically onset within 20-30 minutes of injection. This is a direct consequence of GHSR-1a activation in hypothalamic appetite centers. The hunger is:
- Dose-dependent — Higher doses produce more intense appetite
- Transient — Usually lasts 30-60 minutes
- Difficult to ignore — Many report it as genuinely intense, beyond normal hunger
- More pronounced than other GHRPs — This is GHRP-6's distinguishing side effect
Cortisol Elevation
GHRP-6 stimulates the HPA axis similarly to GHRP-2, causing acute ACTH and cortisol release. At standard doses, the cortisol elevation is transient and typically within physiological ranges. However, repeated high-dose administration could have cumulative effects on cortisol dynamics.
Prolactin Elevation
A modest, dose-dependent increase in prolactin occurs with GHRP-6 administration. Like cortisol, this is generally transient at standard doses. Chronic elevation could theoretically impact libido and reproductive function, though this hasn't been well-characterized in long-term GHRP-6 studies.
Water Retention
Some reports describe mild water retention / bloating, likely related to GH-mediated effects on sodium handling.
Other Reported Effects
- Injection site reactions (mild, transient)
- Numbness or tingling in extremities (uncommon)
- Dizziness (rare, dose-dependent)
- Potential impact on blood glucose — GHSR-1a activation can influence insulin sensitivity
GHRP-6 vs GHRP-2: Quick Comparison
| Parameter |
GHRP-6 |
GHRP-2 |
| Receptor |
GHSR-1a |
GHSR-1a |
| GH Release Potency |
Strong |
Strong |
| Appetite Stimulation |
Intense |
Mild-moderate |
| Cortisol Elevation |
Moderate |
Moderate |
| Prolactin Elevation |
Moderate |
Moderate |
| Cytoprotective Research |
Extensive |
Moderate |
| Clinical Diagnostic Use |
Limited |
Approved (Japan) |
| Half-Life |
~15-30 min |
~15-30 min |
| Standard Dose |
100-200 mcg |
100-200 mcg |
| Best For |
Recovery / appetite support |
GH stimulation with less hunger |
| Synergy with GHRH |
Yes (strong) |
Yes (strong) |
The core difference: GHRP-6 is the hungrier GHRP. If appetite stimulation is desirable (recovery, underweight, post-illness), GHRP-6 has an advantage. If hunger is unwanted, GHRP-2 or ipamorelin may be better choices.
For a much deeper head-to-head analysis, see our Hexarelin deep dive to understand where GHRP-6 sits relative to the most potent GHRP in the family.
Stacking GHRP-6 with GHRH Analogs
The Synergy Principle
The scientific rationale for combining GHRP-6 with a GHRH analog (CJC-1295, Sermorelin, etc.) is well-established:
- GHRP-6 activates GHSR-1a → Gq → PLC → PKC → intracellular calcium
- GHRH analog activates GHRHR → Gs → cAMP → PKA → calcium channel modulation
- Result: Both pathways converge on calcium-dependent GH vesicle exocytosis, producing synergistic output
Veldhuis et al. have documented that the GHRP + GHRH combination produces GH responses 3-10× greater than either peptide alone (Differential pulsatile secretagogue control, 2013).
CJC-1295 as Stacking Partner
CJC-1295 (with or without DAC) is the most commonly discussed GHRH analog for stacking with GHRP-6:
- CJC-1295 with DAC provides sustained GHRH receptor activation over days (Teichman et al., 2006)
- CJC-1295 without DAC (mod GRF 1-29) has a shorter duration, allowing more precise pulse timing
- The combination leverages dual-pathway synergy
For how CJC-1295 compares to Sermorelin as a GHRH stacking partner, see our CJC-1295 vs Sermorelin analysis.
Stacking Considerations
When combining GHRP-6 with GHRH analogs:
- Administer both peptides simultaneously for maximum synergy
- Maintain fasted state for optimal response
- Be aware that the combination may amplify both GH release and side effects (cortisol, hunger)
- The synergy is modulated by age, sex steroids, and body composition
Our Peptide Stacking Guide covers multi-peptide protocols in depth.
GHRP-6 in Stroke and Critical Illness Research
One of the most interesting areas of GHRP-6 research extends well beyond bodybuilding or anti-aging. Cuban research groups have extensively studied GHRP-6 for:
These applications leverage GHRP-6's cytoprotective properties — effects that appear to be at least partially independent of GH release and may involve direct GHSR-1a-mediated anti-inflammatory and anti-apoptotic signaling.
Frequently Asked Questions
How much GHRP-6 should I take?
Clinical research typically uses 1-2 mcg/kg (approximately 100-200 mcg for most adults). This range produces robust GH release. Higher doses produce diminishing returns on GH while increasing side effects, particularly hunger and cortisol elevation.
Why does GHRP-6 make me so hungry?
GHRP-6 activates the ghrelin receptor (GHSR-1a) in the hypothalamus, directly stimulating NPY/AgRP neurons that drive appetite. This is the same pathway ghrelin uses — and GHRP-6 is a particularly effective ghrelin mimetic for orexigenic signaling. The hunger typically peaks 20-30 minutes post-injection and lasts 30-60 minutes.
Is GHRP-6 stronger than GHRP-2?
In terms of GH release, they're comparable at equivalent doses. GHRP-6 produces more intense appetite stimulation. For overall potency in the GHRP family, hexarelin sits at the top — see our Hexarelin guide for details.
Can GHRP-6 be used for weight gain?
GHRP-6's combination of GH stimulation and significant appetite increase makes it relevant in research on weight gain, recovery from illness, and addressing cachexia. The appetite stimulation is a feature in these contexts rather than a side effect.
How long does GHRP-6 take to work?
GH release begins within 15-30 minutes of subcutaneous injection, with peak levels at approximately 30-60 minutes. Appetite stimulation typically begins within 20 minutes. GH levels return toward baseline within 2-3 hours.
Does GHRP-6 need to be taken on an empty stomach?
Yes. Elevated blood glucose, insulin, and free fatty acids significantly blunt the GH response to GHRP-6. Administer 30-60 minutes before eating or 2+ hours after a meal for optimal results.
Can GHRP-6 be combined with other peptides?
Yes — combining GHRP-6 with a GHRH analog (CJC-1295, Sermorelin) is the most evidence-supported stacking approach, producing synergistic GH release through complementary receptor pathways. See our Peptide Stacking Guide for detailed protocols.
What's the difference between GHRP-6 and ipamorelin?
Ipamorelin is a more selective GHSR-1a agonist with minimal cortisol, prolactin, and appetite effects. GHRP-6 produces more GH release but with significantly more hunger and slightly more cortisol/prolactin stimulation. See our GHRP comparison for the full breakdown.
Does GHRP-6 have heart benefits?
Preclinical research suggests GHRP-6 has cardioprotective properties, including protection against doxorubicin-induced cardiotoxicity and ischemia/reperfusion injury. A Phase I/II stroke trial has also been conducted. These effects may be partially independent of GH release.
Summary
GHRP-6 is a potent growth hormone secretagogue with a distinctive profile: strong GH release paired with pronounced appetite stimulation. Its mechanism — GHSR-1a agonism triggering Gq/PLC/PKC signaling — places it in the same receptor family as GHRP-2, hexarelin, and ipamorelin, but its orexigenic potency sets it apart.
Key takeaways:
- Standard dosing: 100-200 mcg (1-2 mcg/kg), 2-3 times daily
- Most distinguishing feature: intense hunger within 20-30 minutes
- Administer fasted for best GH response
- Synergistic with GHRH analogs through complementary signaling pathways
- Emerging research on cytoprotective, cardioprotective, and neuroprotective effects
- Cortisol and prolactin elevation are dose-dependent and generally transient
- Compared to GHRP-2: similar GH release, much more hunger, more cytoprotective research
Whether GHRP-6 or GHRP-2 is the better choice depends on goals. For appetite stimulation in recovery contexts, GHRP-6 has a clear advantage. For GH stimulation with less hunger, GHRP-2 is the standard. For minimal side effects, ipamorelin is the cleanest option.
References
- Bowers CY. Growth hormone-releasing peptide (GHRP). Cell Mol Life Sci. 1998;54(12):1316-29. PMID: 9893708
- Howard AD, et al. A receptor in pituitary and hypothalamus that functions in growth hormone release. Science. 1996;273(5277):974-7. PMID: 8688086
- Kojima M, et al. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402(6762):656-60. PMID: 10604470
- Bowers CY. Unnatural growth hormone-releasing peptide begets natural ghrelin. J Clin Endocrinol Metab. 2001;86(4):1464-9. PMID: 11297568
- Pharmacokinetic study of GHRP-6 in nine male healthy volunteers. Eur J Pharm Sci. 2012;48(1-2):40-6. PMID: 23099431
This article is for educational and informational purposes only. It is not medical advice. GHRP-6 is a research compound — consult a qualified healthcare provider before considering any peptide protocol.