TB-500 is a synthetic 17-amino-acid fragment of Thymosin Beta-4, containing the active actin-binding domain responsible for cell migration and tissue repair. It's a cornerstone of healing peptide protocols, especially when stacked with BPC-157.
Clinical Status: No human trials exist for TB-500 specifically. All protocols are extrapolated from Thymosin Beta-4 research and animal studies. This is not medical advice.
Quick Reference: Standard Protocol
| Parameter |
Standard Protocol |
| Dose |
500 mcg (10 units on insulin syringe) |
| Route |
Subcutaneous injection (systemic — site doesn't matter) |
| Timing |
AM |
| Frequency |
Every day |
| Cycle |
8 weeks on, 8 weeks off |
| Vial size |
10 mg |
| Reconstitution |
2 mL bacteriostatic water → 5,000 mcg/mL |
| Draw amount |
10 units on insulin syringe |
| Storage |
Refrigerate, use within 28 days |
Standard protocol: 500 mcg daily in the morning for 8 weeks, then 8 weeks off. TB-500 works systemically, so injection site location doesn't affect efficacy. For the full TB-500 profile, vendor pricing, and stacking options, see our TB-500 peptide page.
Cycling Details
The standard cycle is 8 weeks on, 8 weeks off. Tissue remodeling and healing effects build over 4-6 weeks and continue through the full 8-week window. The off period allows receptor sensitivity to reset and prevents potential downregulation.
Unlike some peptides, TB-500 protocols use consistent daily dosing throughout the cycle — no loading or tapering needed. The daily protocol is preferred because TB-500's half-life supports once-daily dosing, and consistent levels optimize the cellular repair processes it targets (Kim & Bhatt, 2013).
Note: The standard protocol above follows the cheat sheet. The enhanced protocol below is based on community experience.
| Parameter |
Enhanced Protocol |
| Dose |
2–2.5 mg twice weekly |
| Frequency |
2x per week |
| Weekly total |
4–5 mg (vs 3.5 mg standard) |
| Use case |
Less frequent injections, mimics TB-4 research protocols |
Some users prefer twice-weekly pulsing for convenience. Weekly totals are similar, but daily dosing provides more stable tissue levels.
Routes of Administration
Subcutaneous (standard): Inject anywhere convenient — abdomen, thigh, upper arm. TB-500 distributes systemically regardless of site. Use 29-31 gauge insulin syringe.
Intramuscular: Occasionally used but offers no advantage over subcutaneous for a systemic peptide like TB-500.
Not recommended: Oral (peptide degradation), nasal (no data), topical (molecular weight too large).
Reconstitution Quick Reference
| Vial Size |
BAC Water |
Concentration |
500 mcg Dose |
| 10 mg |
2 mL |
5,000 mcg/mL |
10 units |
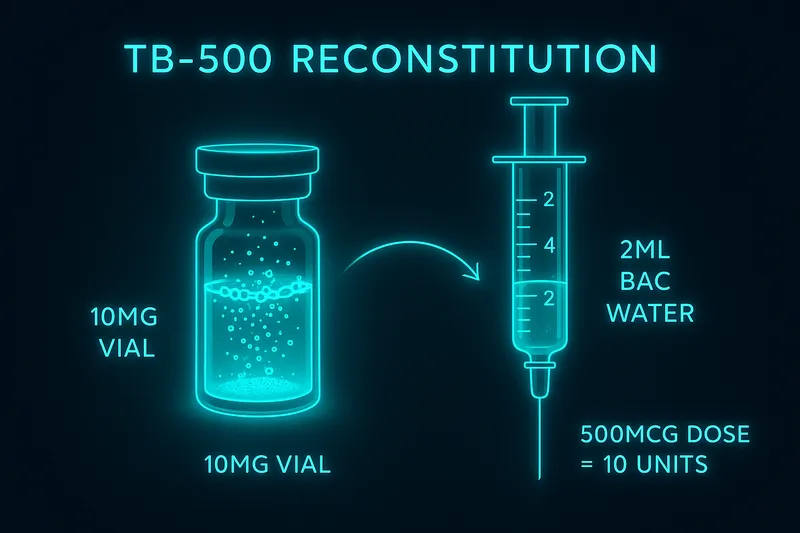
10 mg vial + 2 mL BAC water = 5,000 mcg/mL. Your 500 mcg dose is 10 units on an insulin syringe. One vial lasts 20 days.
Swirl gently — do not shake. Refrigerate at 2-8°C and use within 28 days. For the full step-by-step walkthrough, see the TB-500 Reconstitution Guide.
Where These Numbers Come From
Community TB-500 dosing is extrapolated from Thymosin Beta-4 research, adjusted for molecular weight differences.
Phase I Human Safety (Ruff et al., 2010): IV doses up to 1,260 mg were well-tolerated in healthy subjects with no dose-limiting toxicities — linear pharmacokinetics across the dose range.
Animal Efficacy Studies: Standard research dose of 6-30 mg/kg in rodents. Cardiac protection at 6 mg/kg IV twice weekly (Bock-Marquette et al., 2004).
Scaling logic: TB-500 is the 17-23 amino acid fragment (~845 Da) of full TB-4 (~4,921 Da). Pro-rata scaling from TB-4 protocols of 2-10 mg/week gives 0.34-1.7 mg/week. The community settled on 3.5 mg/week (500 mcg daily) — the middle of this range. The LKKTET motif in TB-500 captures the core actin-binding mechanism at a fraction of the cost (Malinda et al., 1999).
Stacking Protocols
TB-500 + BPC-157 (The Gold Standard Healing Stack)
| Peptide |
Dose |
Route |
Timing |
Purpose |
| TB-500 |
500 mcg daily |
SC (anywhere) |
AM |
Cell migration, actin remodeling |
| BPC-157 |
250-500 mcg daily |
SC (near injury) |
AM or PM |
Angiogenesis, growth factors |
Run both for 8 weeks on, 8 weeks off. Or use the pre-mixed Wolverine Stack for convenience.
TB-500 + GHK-Cu
| Peptide |
Dose |
Route |
Timing |
Purpose |
| TB-500 |
500 mcg daily |
SC |
AM |
Cell migration, systemic repair |
| GHK-Cu |
1-3 mg 2x weekly |
SC |
AM |
Collagen synthesis, gene activation |
Good for skin healing, anti-aging, and cosmetic recovery protocols.
Side Effects & Safety
- Injection site irritation — mild redness, transient
- Mild fatigue — first week of use, typically resolves
- Transient muscle/joint aches — as healing ramps up
- Occasional headaches — uncommon
- Mild nausea — rare
- Theoretical cancer concern — TB-500 promotes cell migration; no studies show tumor promotion, but caution warranted with existing cancers
- No long-term human data — TB-500 specifically has no direct human trials
Frequently Asked Questions
What is the standard TB-500 dose?
The standard protocol is 500 mcg daily via subcutaneous injection in the morning, cycled 8 weeks on / 8 weeks off. Use a 10 mg vial with 2 mL BAC water — 500 mcg equals 10 units on an insulin syringe.
Does injection site matter with TB-500?
No — TB-500 works systemically regardless of injection site. Unlike BPC-157 where some people inject near injuries, TB-500 circulates throughout the body. Inject wherever is convenient: abdomen, thigh, or arm.
How does TB-500 differ from full Thymosin Beta-4?
TB-500 is the active 17-23 amino acid fragment containing the key LKKTET actin-binding domain. Full TB-4 has 43 amino acids with additional signaling sequences. TB-500 captures most healing effects at a fraction of the cost.
How long should a TB-500 cycle last?
8 weeks on, 8 weeks off. Tissue remodeling effects build over 4-6 weeks and continue through 8 weeks. Cycling prevents potential receptor downregulation.
Can TB-500 and BPC-157 be taken together?
Yes — this is the most popular healing peptide combination. They work through different mechanisms (TB-500: cell migration and actin remodeling; BPC-157: angiogenesis and growth factors) and are highly complementary.
How do I reconstitute TB-500?
Add 2 mL bacteriostatic water to a 10 mg vial (5,000 mcg/mL). 500 mcg = 10 units on an insulin syringe. Swirl gently, refrigerate, use within 28 days.
References
| Citation |
Topic |
PMID |
| Ruff et al., Wound Repair Regen (2010) |
Thymosin Beta-4 Phase I human safety, IV doses up to 1,260mg |
20536472 |
| Malinda et al., Proc Natl Acad Sci (1999) |
TB-500 actin-binding domain, LKKTET sequence mechanism |
10469335 |
| Bock-Marquette et al., Nature (2004) |
Thymosin Beta-4 cardiac protection, 6 mg/kg dosing in mice |
15565145 |
| Kim & Bhatt, Annu Rev Med (2013) |
TB-500 mechanisms, cell migration, tissue repair review |
23523891 |
| Philp et al., J Cell Sci (2004) |
Actin sequestration and cell motility mechanisms |
15252124 |
| Sosne et al., Invest Ophthalmol Vis Sci (2010) |
Anti-inflammatory effects and wound healing |
20207966 |
For educational and research purposes only. This is not medical advice. TB-500 has no FDA-approved indications and is not intended for human consumption.